Listeners:
Top listeners:
-
 play_arrow
play_arrow
Radio Today Radio Today
-
 play_arrow
play_arrow
Afternoon Finance Mike Stroud
-
play_arrow
Afternoon Finance Mike Stroud
music_note
Vertigo

WHAT IS VERTIGO AND WHAT CAUSES IT?

Vertigo vs. Dizziness
Vertigo is not the same as dizziness. Feeling dizzy means that you’re lightheaded, weak, or unsteady on your feet. Vertigo is a sensation of spinning and feeling off balance and dizzy. The causes also differ. Dizziness can result from a drop in blood pressure, medications you take, a vision problem, or a mental health condition. Vertigo occurs with conditions such as migraine, head injury, Meniere’s disease, and the movement of crystals in your inner ear that keep you balanced.
Types of Vertigo
Vertigo has two main types: peripheral and central. The difference between the two types is what causes them.
Peripheral vertigo
This is the most common type of vertigo. It happens because of a problem with your inner ear or the vestibular nerve in your brain. These structures help you stay balanced. One cause of peripheral vertigo is benign paroxysmal positional vertigo (BPPV) — an inner ear disorder. BPPV causes vertigo when you move your head a certain way, such as tipping it backward.
Central vertigo
This less common type of vertigo stems from a problem in the brain, such as a stroke or infection. It causes more severe symptoms, such as difficulty walking.
Vertigo Causes
Vertigo often happens because of an inner ear problem. Some of the most common causes include:
Benign paroxysmal positional vertigo (BPPV). This inner ear disorder happens when tiny calcium particles (canaliths) get dislodged from their normal location and collect in the inner ear. The inner ear sends signals to the brain about your head and body movements to help you keep your balance.
Meniere’s disease. This inner ear disorder may be caused by a buildup of fluid and changing pressure in the ear. It can cause episodes of vertigo along with ringing in the ears (tinnitus) and hearing loss.
Vestibular neuritis or labyrinthitis. This inner ear problem is usually related to a viral infection such as chickenpox, measles, or hepatitis. The infection inflames nerves that help your brain keep you balanced.
Stress and Vertigo
Dizziness and a spinning sensation can be symptoms of stress and anxiety. The same areas of the brain may be involved in producing feelings of anxiety and dizziness. Stress is also a risk factor for labyrinthitis, a cause of vertigo.
Vertigo can also be caused by:
- A head or neck injury
- Brain problems, such as a stroke or tumour
- Certain medications that cause ear damage, including some antibiotics, heart drugs, and anti-inflammatory medicines
- Migraine headaches
- Ear infection
- Acoustic neuroma, a noncancerous tumour in the ear
- Stroke
- Dehydration
- Irregular heart rhythms
- Ear surgery
- Low blood pressure
- Diseases such as multiple sclerosis or diabetes
- Otosclerosis, abnormal bone growth in the middle ear
- Headache
- Sweating
- Ringing in the ears or hearing loss
- A feeling of fullness in the ear
- Double vision
- Difficulty swallowing
- Slurred speech
- Weakness in your arms and legs
- Trouble moving your face
Each vertigo attack can last from a few seconds to several hours, but the feeling of being off-balance may stay with you for much longer. For people with severe vertigo, attacks can sometimes last for days or months.
One or more of these tests may be necessary to find the cause of your vertigo:
Hearing tests. These tests check for a problem with the nerve in your inner ear.
Caloric testing. An audiologist stimulates your inner ear with cold or warm air to see if it makes you dizzy. This test can detect damage to the acoustic nerve.
Electronystagmography. This test checks your eye movements to see how well the vestibular nerve and other nerves in your inner ear and brain are working.
Fukuda-Unterberger test. You march in place for 30 seconds with your eyes closed. If you turn or lean to one side, you could have an inner ear problem.
Head impulse test. Your doctor moves your head from side to side while you focus on the wall or another unmoving object. This test can detect a problem with the balance system in your inner ear.
Romberg’s test. You stand still with your feet together and your eyes closed. If you feel unsteady, it could be from a problem with your brain or spinal cord.
Vestibular test battery. These tests check for problems with the vestibular system in your inner ear.
Imaging tests. MRI and CT scans can detect problems in your inner ear or brain.
There are many options for treating vertigo:
Vestibular rehabilitation
This is a type of physical therapy aimed at helping strengthen the vestibular system. This system sends signals to your brain about your head and body movements. Your doctor may recommend vestibular rehabilitation if you have repeated bouts of vertigo. It helps train your other senses to compensate for vertigo.
Surgery
Some conditions that cause vertigo require surgery to fix. If vertigo is caused by a more serious underlying problem, such as a tumour or injury to the brain or neck, treating these problems may help to relieve the vertigo.
Vertigo medication
Motion sickness medicines such as meclizine (Antivert, Bonine) or dimenhydrinate (Dramamine) can ease vertigo symptoms such as nausea and dizziness. If an infection or inflammation is the cause of your vertigo, you may need steroids to reduce swelling or antibiotics to get rid of the infection. For Meniere’s disease, diuretics (water pills) reduce pressure from fluid buildup.
How to Stop Vertigo
You might not be able to stop vertigo with at-home methods, but you can ease symptoms with a few self-care tips. Here are a few vertigo home remedies you can try:
- Drink more water, sports drinks, or other fluids. Dehydration can make vertigo worse.
- Control stress. Practice relaxation techniques such as deep breathing or meditation to calm anxiety before it can affect your balance.
- Limit caffeine, alcohol, salt, and tobacco. These substances make dizziness worse.
- Lie in a dark, quiet room. This may help to relieve the spinning.
- Move slowly. Walk, get out of bed, and turn your head slowly to prevent dizziness. Use a cane if you need it to avoid falls. Sit or lie down as soon as you start to feel dizzy. Bend from the knees instead of leaning over from the waist when you pick something up.
How to Cure Vertigo Permanently
There is no cure for vertigo. While some people have a single episode and never experience the spinning feeling again, others may have many attacks.
If you have repeated bouts of vertigo, talk to your doctor about ways to treat the cause and relieve your symptoms.
- Chest pain
- Trouble walking
- Numbness or weakness in your arms or legs
- Fever higher than 100.4 F / 38ºC
- Vision changes such as double vision
- Weakness in an arm or leg
- Rapid or irregular heartbeat
- Sudden, severe headache
- Slurred speech
- Vomiting that doesn’t stop
Fainting or seizures
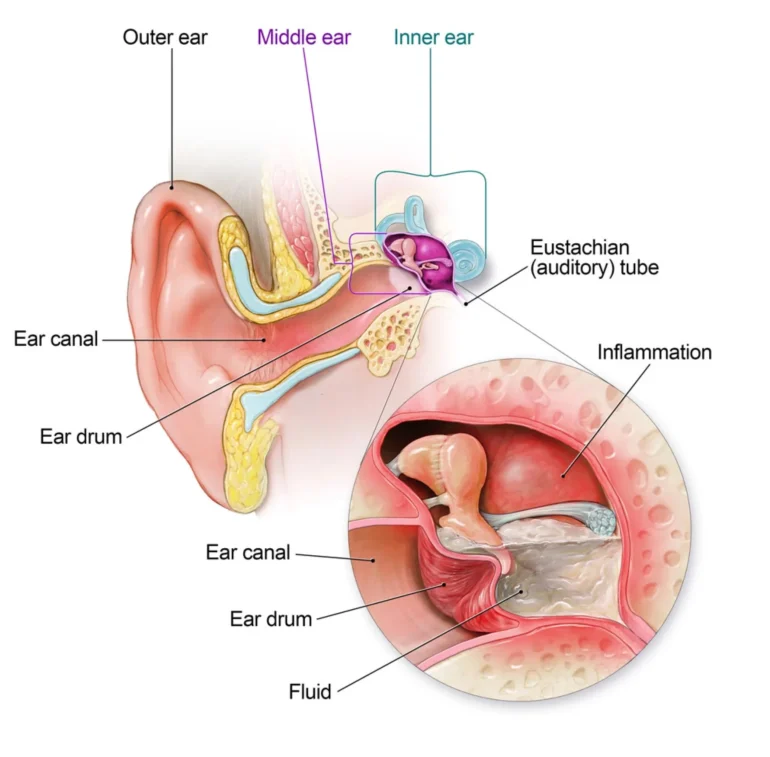
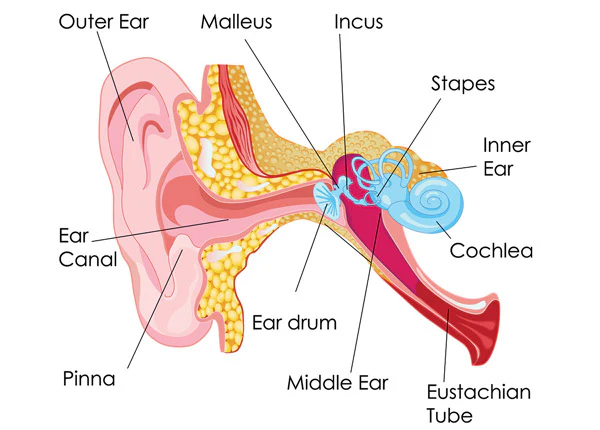
Inner ear disease and vertigo
Many different factors can affect the inner ear and cause vertigo. One way to distinguish them is by the duration of the dizziness.
SHORT-LIVED EPISODES OF DIZZINESS (FEW SECONDS TO MINUTES)
An extremely common type of vertigo is benign positional vertigo. This is typically a very sudden onset of dizziness, which settles rapidly after a few seconds or at most a couple of minutes.
It is often started off by the person suddenly looking upwards or sideways, and some people get it when they turn over in bed. In between attacks, the sufferer feels entirely normal. It is probably caused by a little piece of lining coming loose in the inner ear and floating into the balance receptor, causing a sudden increase in nerve stimulus to the brain.
Sometimes the attacks start following a whiplash injury or other head injury, but often there appears to be no reason that they should have started. The attacks usually disappear with time.
Medicines do not help, but a manoeuvre known as Epley’s Manoeuvre can be extremely effective in some patients. This can be carried out either by the ear nose and throat surgeon or physiotherapy department, depending on the hospital.
MEDIUM LENGTH EPISODES OF DIZZINESS (HALF-HOUR TO SEVERAL HOURS)
These types of vertigo are rarer and are thought to be due to an increase in pressure of the fluid in the inner ear, although nobody really knows for sure.
Menière’s disease or endolymphatic hydrops result in episodes of severe vertigo that can last up to several hours. The dizzy episodes are usually linked with vomiting, and the sufferer can often tell an episode is about to start because he or she notices a drop in their hearing, a feeling of fullness in the ear and some tinnitus. The hearing recovers once the vertigo has settled, but may gradually deteriorate with time.
Treatment of Menière’s disease can involve medicines and, more rarely, surgery, but this will be organised by your local ear nose and throat department once the diagnosis of Menière’s disease has been made.
LONGER EPISODES OF DIZZINESS (DAYS TO WEEKS)
An infection of the inner ear (labyrinthitis) or an inflammation of the balance nerve (vestibular neuronitis) can give rise to severe rotatory dizziness for up to two to three weeks, with a slow return to normal balance which can take a further few weeks.
Again, the initial episode is often associated with vomiting and the patient can be bed-bound because the dizziness is so severe. This is best treated at first with a vestibular sedative such as Stemetil, but any treatment should be stopped quite quickly to allow the brain to compensate and recover from the dizziness. Recovery is much quicker in the long run if treatment with anti-dizziness medicines is not prolonged.
The inner ear may be ‘suppressed’ (or made sleepy) by the use of drugs such as Stemetil or Stugeron. These drugs reduce the overactivity of the balance organ and so reduce the dizziness and vomiting that can occur in inner ear problems.
However, they are not a long-term solution and should be used for as short a time as possible because they prolong the time taken for the body to readjust after the vertigo.
Menière’s disease
This is a longer term disease and there are two aims of treatment. One is to treat the acute episodes of dizziness with vestibular sedatives (see above), and the other is to try to reduce the frequency of the dizzy episodes.
Frequently advice will be given to restrict intake of salt, caffeine and alcohol, which can help some patients with Menière’s disease. Increasing the bloodflow of the inner ear may help and so drugs like Betahistine (Serc) are often prescribed.
Some people with Menière’s disease may benefit from surgery if the episodes of vertigo are frequent and disabling and not responding to medical treatment.
When surgery is needed
Surgery may be advised if medical treatment proves ineffective and the episodes of vertigo are disabling. The options range from those such as the simple insertion of a grommet through to operations which completely destroy the inner ear, or divide the nerves leading from the inner ear to the brain.
Unfortunately, many (although not all) effective surgical operations also destroy the hearing of that ear and so the vertigo is usually severe before a patient opts to undergo such treatment.
Because there are so many different causes of vertigo, there are several different operations and so it would take too much space to detail them all here, but your ear nose and throat consultant will go through them with you.
New treatments
There are always new treatments being developed and there is very encouraging progress being made using drugs delivered directly into the ear which selectively destroy the inner ear balance mechanisms without affecting hearing.
Further work is still to be undertaken in this area and will no doubt result in improved techniques for the control of vertigo in patients who are long-term sufferers. Anyone suffering from persistent recurrence of vertigo should consult their doctor in order to find the cause and to arrange effective treatment.
By D Bowdler and R Lloyd Faulconbridge, University Hospital Lewisham
Similar posts


Featured post
Latest posts
Current show
Upcoming shows















Post comments (0)